Instructions for risk derivatives of silica in silicone breast implants
This chapter examines the Institute of Medicine (IOM) from 1999 about silicone breast implants and the possible activation of T cells, white blood cells that are crucial to the immune system. Activation of T-cells by substances such as pyrogenic Although the IOM report cites studies that did not find convincing evidence for T-cell activation by silicone or silica, it trivializes crucial signals, such as the toxicity of silica to macrophages. We show how these clues were ignored.
Point 1: The IOM ignores the specific risks of pyrogenic amorphic silica
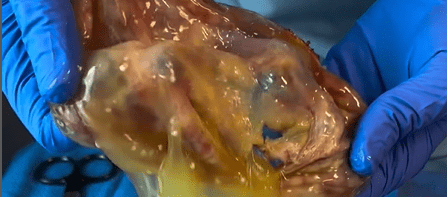
In general terms, the IOM speaks of "silica" without distinguishing between crystalline silica (as in quartz) and pyrogenic amorphic silica . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . This is a major flaw, because pyrogenic amorphic silica has unique properties: It consists of nanoparticles that become highly reactive and can cause inflammation when silicone is degraded. The IOM states that "there is no evidence that women are exposed to silica via implants," but this is not correct and is painfully degraded by the photo (top) of a silicone breast implant, disintegrated to a blubber mass.
Point 2: Selective and biased criticism of the IOM
The IOM criticises studies such as Ojo-Amaize (1994) and Smalley (1995a, 1995b) for methodological problems such as inconsistent controls and non-reproductive results. Although some criticisms are justified, this fits into a pattern: The IOM systematically rejected studies that showed risks, while studies that found no risk (often with conflicts of interest) were accepted. For example, an independent test by Young (1996b) showed inconsistent results, but this doesn't mean that silica doesn't cause T-cell activation. The IOM should have encouraged this, but wrote these studies down completely. In addition, the IOM recognises that silica is activating macrophages that cause inflammation, but does not remove it as irrelevant, without examining the specific effects of pyrogenic silica. This is a missed opportunity, because macrophages can activate T cells, as Shanklin and Smalley (1998) showed.
Point 3: Complaints from women correspond to silica effects
Smalley et al. (1995b) found that 91.3% of women with implants and health complaints had an increased T-cell response to silica. This is consistent with our hypothesis that pyrogenic amorphic silica causes immune reactions. The IOM dismisses this finding as non-specific, but ignores that this is exactly what you would expect from exposure to pyrogenic silica. Shanklin and Smalley (1998) showed that silica causes T-cell reactions, which fits the experiences of women.
Point 4: The IOM ignores wider evidence of immune responses
Studies such as Ellis et al. (1997b) found that women with implants had increased T-cell reactions to connective tissue components, such as collagen, suggesting an autoimmune reaction. Although Ellis did not find a direct response to silica, this may be indirectly related: silica activates macrophages, which can stimulate T cells. Katzin et al. (1996) found activation markers on T cells in breast tissue of women with implants, indicating a local immune response. The IOM dismisses these findings as insignificant, but they support our point that implants cause immune reactions, possibly via silica. The IOM focuses too narrowly on whether silica is a "clear antigen," while indirect mechanisms are also relevant.
Point 5: Lack of long-term studies
The IOM recognises that more research is needed by highlighting the problems of the studies, but completely rejects the risk derivatives of silica rather than encouraging further research. This fits with our criticism that there is a shocking lack of research into pyrogenic silica: of the 12,204 studies on breast implants on PubMed, only 2 are about pyrogenic silica. Studies such as Ciapetti et al. (1995), which found an increased T-cell response to silicone gel, were rejected by the IOM due to methodological problems. This underlines our point that too little serious research has been done.
Point 6: Animal studies and delayed hypersensitivity
Studies such as Narini et al. (1995) and Kossovsky et al. (1998) investigated immune responses in animals, but found no specific response to silicone. The IOM uses this to conclude that silicones are not T-cell antigens. However, these studies used silicone gel, not pyrogenic amorphic silica, which is our central point. This makes the conclusions of the IOM irrelevant to the risks related to silica. Brantley et al. (1990) and Klikken et al. (1991) also found no immune response in animals, but did not specifically investigate silica, which reinforces our point that the IOM overlooked these risks.
Key findings of Shanklin and Smalley
In several studies, Shanklin and Smalley have demonstrated the risks of silica in silicone implants. Below are some crucial quotes from Immunology of Silicones (translated into Dutch):
- The role of silica in inflammations: "Because of the presence of pyrogenic silica in the elastomer, it is relevant to discuss the immunology of SiO2 (silica). It has been known for years that certain forms of silica cause strong fibrosis. This starts a process where macrophages absorb the silica particles and secrete substances that create scar tissue, such as TNF-α and TGF-β. Elastomer shell components can thus cause an inflammatory reaction via macrophages."
- Presence of silica in tissues: "The other important foreign material in tissues around implants is silica. A limitation is that polarisation microscopy only detects crystalline silica. In our samples, we found silica in 76.2% and 86.7% of cases, slightly less common than silicone. There is evidence that amorphic and pyrogenic amorphic silica are as reactive as crystalline silica. The evidence for the role of silica comes mainly from T-cell reactivity, which is more sensitive than microscopic methods. We need a method to measure the total amount of silica in the hairstyle. Approximately 26% of the samples had a less thick hairstyle, and some had more mineralization (15.7%), suggesting deposition of substances such as calcium . Silica is a known causer of fibrosis, similar to pulmonary diseases such as siliconosis."
- T-cell activity and immune responses: "An important aspect of immune responses to silicone implants concerns T-cells. Silica may be a causer, as Shanklin et al. showed: They found silica in hairstyles and showed that blood cells of women with implants are hypersensitive to silica. Other studies, such as those of O.H.Hanlon et al., found local immune responses in hairstyles, and Young et al. found a link to certain immune profiles (HLA-DR53) in women with complaints."
Disclaimer:
The information on this website is intended for informational purposes and is based on carefully collected scientific research. The topics and hypotheses discussed have not yet been widely recognised within the medical community. We are not doctors and do not give medical or legal advice. No rights can be derived from the content of this website. Stichting SVS accepts no liability for any consequences, damage, complaints or legal proceedings arising from the use of this information.

